
Human performance optimization (HPO) is a capability-based approach that focuses on health and performance improvements key to optimizing Service Members’ performance of their core tasks (CTs) or primary duties. CTs are important and contribute to the successful execution of the unit’s mission essential task list (METL). HPO accomplishes this by expanding and shifting the traditional spectrum of care to move beyond health (such as weight management and disease prevention) and towards building mission-focused capabilities (such as improved marksmanship).
The HPO spectrum is presented as a capability-based continuum and a job-focused relationship between health and performance. The phases at the top of the HPO Spectrum graphic below (performance sustainment, performance enhancement, and health sustainment) represent a Service Member’s abilities to perform at their job and sustain their health. The colored bullets at the bottom are the actions needed to move left towards optimal performance. Although every Service Member will move through this spectrum over their career at some point, the goal is to keep them performing optimally.
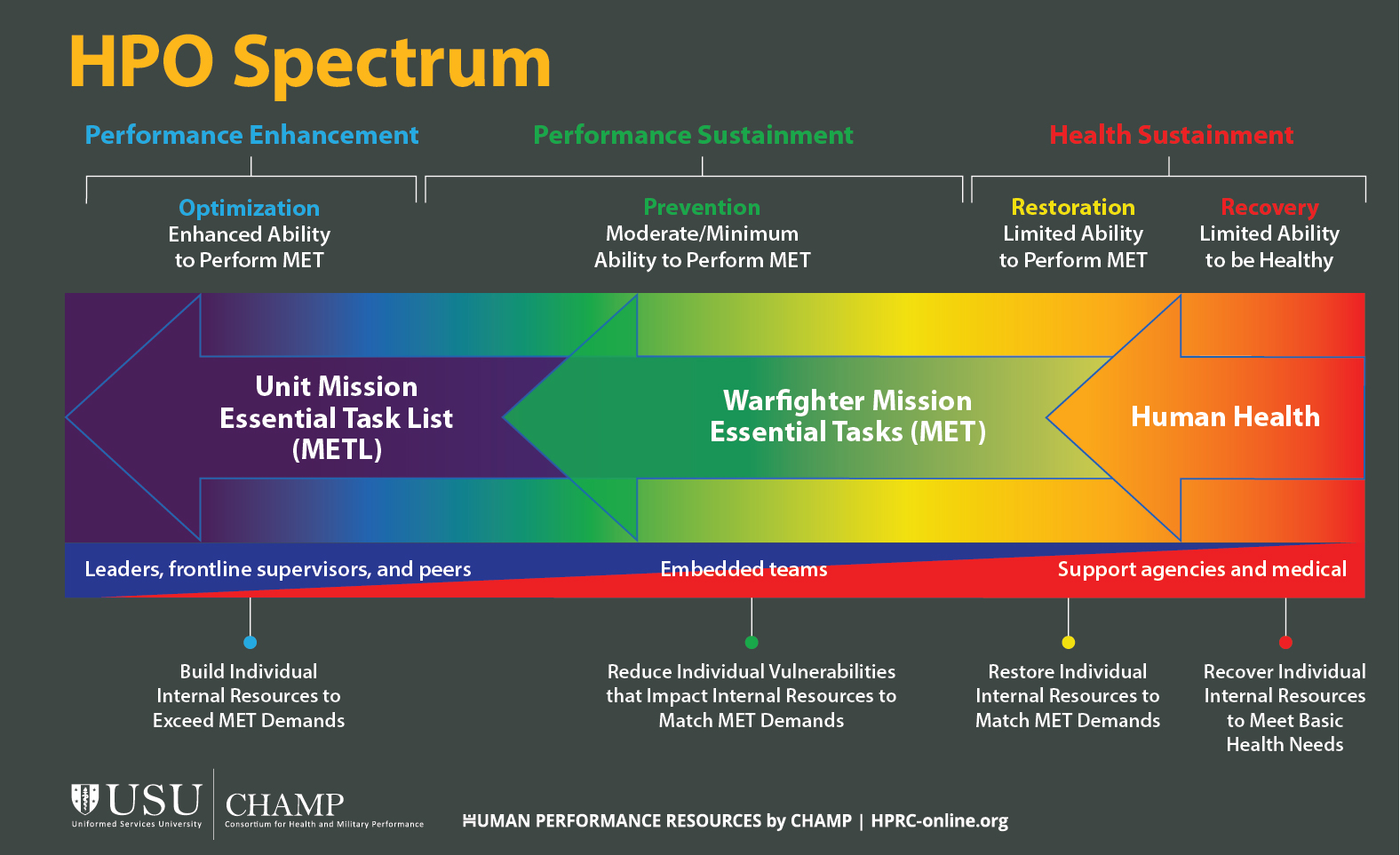
Performance sustainment phase (Green)
This phase represents Service Members who first join the military (or are fully recovered from a prior injury or illness), meet all of the milestones of health sustainment, and have the minimum-to-moderate abilities to perform their CTs within their units. In this performance-sustainment stage, the goal is to reduce potential job-related vulnerabilities that could push them towards the right of the spectrum, negatively impacting their performance and health.
For example, a particular CT for a USMC Artilleryman military occupational specialty (MOS) would require lifting a 95-pound, 155 mm artillery round, carrying it 5 meters, and placing it in a howitzer loading tray 5 times in 75 seconds. Actions taken in the area of injury prevention are to safely maximize physical readiness tailored to meet the physical demands of the job. Physical training should emphasize maximizing muscular strength for lifting and carrying the round, and core stability and muscular endurance to move efficiently and reduce the risk of injury during that task. It’s also important to focus on anaerobic power and cardiorespiratory endurance to complete those repetitions within the set time.
Vulnerabilities are possible in every domain of Total Force Fitness (TFF), not just the physical domain. Some military occupations expose Service Members to potentially traumatic events. For example, military first responders and dispatchers—such as USAF Fire Protection, Army Combat Medics, or USCG Command Center personnel—perform CTs that save lives, aid personnel in distress, or coordinate responses to distress calls. Repeated exposure can lead to mental and emotional stressors over time, which can contribute to reduced CT performance levels. With these occupations, resources should focus on psychological preparedness and injury prevention to address the unique mental demands of their CTs. Approaches such as stress inoculation training can aid in psychologically preparing Service Members to better manage exposures that come with their occupations.
Performance enhancement phase (Purple)
This phase focuses on building CT-specific capabilities to exceed the demands of Service Members’ occupational CTs. For instance, certain occupations exist within the military such as a USMC Infantry Rifleman and Army Infantryman for which marksmanship is a critical CT. Basic CT performance would require enough focus to not blindly pull the trigger. Then you can apply psychological performance-enhancement strategies to improve marksmanship skills. Guided imagery might enhance trigger-squeeze competencies, and self-regulation skills such as focused breathing can improve your ability to manage your body’s physiological responses to improve target acquisition.
Health sustainment phase (Yellow/Red)
At some point in their careers, Service Members will become injured as a result of their job. Both the restoration and recovery stages are in the “health sustainment” phase because resources are being directed towards your ability to maintain basic health functions. This phase includes those who have sustained some type of injury (physical, mental, emotional, or moral) that impacts their ability to perform basic CT functions. In addition, they’re limited in their ability to be healthy, which means they’re not in a state of well-being across all TFF domains. This doesn’t just refer to illness or injury. On the HPO spectrum, you’re fully out of the red zone and transitioning towards the green as your ability to perform your CTs is restored. The restoration stage isn’t permanent while a Service Member is in a state of recovery. Depending on the severity of the injury, CT continued exposures, and the use of self-help or professionally-guided strategies to minimize the impact of the injury, the Service Member will either transition left to the performance sustainment phase or right to the recovery stage requiring advanced care. Depending on the military occupation and the sensitivity of the CT during the restoration stage, healthy Service Members could be placed on “limited duty” status and removed from their primary duties for a period of time. For instance, USAF Security Forces members returning from deployment serving in a combat role “out of the wire” would go through the Deployment Transition Center and be placed on limited duty upon arriving home to help with acclimating back from the kinetic operations of their deployment.
If Service Members' conditions worsen and they transition to the recovery phase, the primary focus is on their health and retention. In most cases, they are removed from all primary duties, and all resources and services are directed at treating the injury and meeting basic health needs.
Strategic HPO
The HPO model isn’t just for the individual Service Member to use to optimize their performance or for health and performance personnel to target their efforts. It’s also a model for leaders to optimize their units’ mission capabilities and readiness. Since HPO uses a unit’s METLs and Service Member’s CTs as foundational to decision-making, it will ensure that health and performance resources are aligned to the needs of both the unit and its diverse career fields to optimize their mission-specific capabilities. For example, a USAF Intelligence Squadron Commander—whose Geospatial Intelligence Analyst’s CTs require them to be seated for 10–12 hours in a dark, windowless environment—could use the HPO model to identify health data trends specific to the performance of their CT (performance sustainment phase) to improve the targeting of embedded health and performance team service delivery. Data trends might suggest vitamin D deficiencies and higher rates of lower back, head, and neck pain. Job tasks might also require sustained periods of cognitive focus. Embedded service delivery might choose to work closely with unit and installation support agencies to improve ergonomics and lighting, develop a tailored physical fitness program, and possibly explore nutrition optimization, vitamin D supplementation, and mental skills training to boost focus. Finally, the leader could use this experience to shape internal processes and policies to improve collaboration across stakeholders, ensure gains are sustained, and support operational return on investment.
Finally, HPO resources should ideally address all domains of the TFF framework: social, physical, nutritional, medical and dental, psychological, environmental, spiritual, and financial fitness. Read CHAMP’s “Total Force Fitness for the 21st Century: A New Paradigm” and Chairman of the Joint Chiefs of Staff Instruction (CJCSI) 3405.01: Chairman's Total Force Fitness Framework to learn more.